Are Shoe Lifts The Ideal Solution To Leg Length Discrepancy
There are actually not one but two different kinds of leg length discrepancies, congenital and acquired. Congenital means you are born with it. One leg is structurally shorter compared to the other. As a result of developmental periods of aging, the brain picks up on the stride pattern and identifies some variance. Your body typically adapts by tilting one shoulder to the "short" side. A difference of less than a quarter inch is not blatantly irregular, doesn't need Shoe Lifts to compensate and typically does not have a profound effect over a lifetime.

Leg length inequality goes largely undiscovered on a daily basis, however this problem is easily fixed, and can reduce quite a few cases of lumbar pain.
Treatment for leg length inequality usually involves Shoe Lifts. Most are affordable, frequently priced at less than twenty dollars, compared to a custom orthotic of $200 or maybe more. When the amount of leg length inequality begins to exceed half an inch, a whole sole lift is generally the better choice than a heel lift. This prevents the foot from being unnecessarily stressed in an abnormal position.
Low back pain is the most common ailment affecting men and women today. Over 80 million people have problems with back pain at some point in their life. It's a problem that costs companies millions of dollars annually as a result of time lost and productivity. Innovative and better treatment solutions are always sought after in the hope of reducing the economic influence this issue causes.

Men and women from all corners of the world suffer from foot ache as a result of leg length discrepancy. In most of these cases Shoe Lifts are usually of immense help. The lifts are capable of decreasing any pain and discomfort in the feet. Shoe Lifts are recommended by many skilled orthopaedic practitioners".
So as to support the body in a well balanced manner, feet have got a critical role to play. In spite of that, it can be the most overlooked zone of the body. Some people have flat-feet meaning there is unequal force placed on the feet. This will cause other parts of the body including knees, ankles and backs to be affected too. Shoe Lifts ensure that suitable posture and balance are restored.
Leg length inequality goes largely undiscovered on a daily basis, however this problem is easily fixed, and can reduce quite a few cases of lumbar pain.
Treatment for leg length inequality usually involves Shoe Lifts. Most are affordable, frequently priced at less than twenty dollars, compared to a custom orthotic of $200 or maybe more. When the amount of leg length inequality begins to exceed half an inch, a whole sole lift is generally the better choice than a heel lift. This prevents the foot from being unnecessarily stressed in an abnormal position.
Low back pain is the most common ailment affecting men and women today. Over 80 million people have problems with back pain at some point in their life. It's a problem that costs companies millions of dollars annually as a result of time lost and productivity. Innovative and better treatment solutions are always sought after in the hope of reducing the economic influence this issue causes.
Men and women from all corners of the world suffer from foot ache as a result of leg length discrepancy. In most of these cases Shoe Lifts are usually of immense help. The lifts are capable of decreasing any pain and discomfort in the feet. Shoe Lifts are recommended by many skilled orthopaedic practitioners".
So as to support the body in a well balanced manner, feet have got a critical role to play. In spite of that, it can be the most overlooked zone of the body. Some people have flat-feet meaning there is unequal force placed on the feet. This will cause other parts of the body including knees, ankles and backs to be affected too. Shoe Lifts ensure that suitable posture and balance are restored.
The Best Way To Treat Posterior Calcaneal Spur

Overview
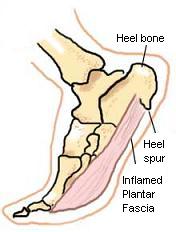
The two most common causes of pain in the bottom of the heel, the arch, or both the heel and the arch, are heel spurs and plantar fasciitis. A Heel Spur is a piece of calcium or bone that sticks out from the bottom of the heel bone, and lies within the fibers of the plantar fascia. When walking, the spur digs into the plantar fascia and causes small micro-tears in the plantar fascia. This produces inflammation and pain in the heel, which at times may radiate into the arch.
Causes
The cause of heel spurs is excessive strain placed on the plantar fascia over a long period of time, as a result of different factors. These factors include incorrect gait, being overweight, ageing or being in a job that requires a lot of standing on hard floors. It is usually a combination of any of these factors that will bring on the development of heel spurs.
Symptoms
The vast majority of people who have heel spurs feel the asscociated pain during their first steps in the morning. The pain is quite intense and felt either the bottom or front of the heel bone. Typically, the sharp pain diminishes after being up for a while but continues as a dull ache. The pain characteristically returns when first standing up after sitting for long periods.
Diagnosis
The diagnosis of heel pain and heel spurs is made by a through history of the course of the condition and by physical exam. Weight bearing x-rays are useful in determining if a heel spur is present and to rule out rare causes of heel pain such as a stress fracture of the heel bone, the presence of bone tumors or evidence of soft tissue damage caused by certain connective tissue disorders.
Non Surgical Treatment
In many cases treatment is non-surgical and can relieve pain, but may take from three months to a year to fully recover. Performing stretching exercises to help relax the tissues in the heel as well as rest, icing, and over-the-counter anti-inflammatory or prescription medications can help ease symptoms. Customized orthotics or shoe inserts to position and cushion your heel can help.
Surgical Treatment
Sometimes bone spurs can be surgically removed or an operation to loosen the fascia, called a plantar fascia release can be performed. This surgery is about 80 percent effective in the small group of individuals who do not have relief with conservative treatment, but symptoms may return if preventative measures (wearing proper footwear, shoe inserts, stretching, etc) are not maintained.
Prevention
You can help prevent heel spur symptoms from returning by wearing the proper shoes. Customized orthotics and insoles can help relieve pressure. It is important to perform your exercises to help keep your foot stretched and relaxed.
Find Out How To Protect Against Calcaneal Spur

Overview
A heel spur is a bony projection at the base of the heel bone, as defined by the website webmd.com. Heel spurs are often accompanied by plantar fasciitis, the inflammation of the soft tissues surrounding the spur, and that is what causes the pain in those who suffer from this condition. To cure or remove a heel spur you will need to see a podiatrist; however, there are some natural remedies and exercises that may help.
Causes
Diseases such as arthritis may lead to chronic inflammation in the tissue surrounding the heel and over time this can lead to the accumulation of calcium deposits. Ankylosing spondylitis, for example, is one particular form of arthritis that frequently develops along with heel spurs. This condition can damage bones all over the body and even lead to the fusion of spinal vertebrae.
Symptoms
Symptoms of heel spur syndrome often include pain early in the morning or after rest, as you take the first few steps. It may also include severe pain after standing or walking long hours, especially on hard cement floors. Usually more pain exist while wearing a very flat soled shoe. A higher heel may actually relieve the pain as an arch is created. The pain is usually sharp, but can also be a dull ache. The pain may only be at the bottom of the heel, or may also travel along the arch of the foot.
Diagnosis
A thorough medical history and physical exam by a physician is always necessary for the proper diagnosis of heel spurs and other foot conditions. X rays of the heel area are helpful, as excess bone production will be visible.
Non Surgical Treatment
Heel pain may be associated with a heel spur, however the heel pain is usually due to plantar fasciitis, rather than a heel spur, so treatment is usually directed at the plantar fasciitis itself. Treatment usually involves application of ice to reduce pain and inflammation, special stretching exercises, and pain-relieving or anti-inflammatory medicines. Night splints or orthotics may be recommended. It may help to avoid the activities that aggravate pain, such as long walks and running. Surgery is very rarely recommended and only after other measures fail.
Surgical Treatment
Surgery is used a very small percentage of the time. It is usually considered after trying non-surgical treatments for at least a year. Plantar fascia release surgery is use to relax the plantar fascia. This surgery is commonly paired with tarsal tunnel release surgery. Surgery is successful for the majority of people.
Prevention
You can prevent heel spurs by wearing well-fitting shoes with shock-absorbent soles, rigid shanks, and supportive heel counters; choosing appropriate shoes for each physical activity; warming up and doing stretching exercises before each activity; and pacing yourself during the activities. Avoid wearing shoes with excessive wear on the heels and soles. If you are overweight, losing weight may also help prevent heel spurs.
Treatment For Bursitis Of The Foot
Overview
Bursitis is the painful inflammation of the bursa, a padlike sac found in areas subject to friction. Bursae cushion the movement between the bones, tendons and muscles near the joints. Bursitis is most often caused by repetitive movement and is known by several common names including weaver's bottom, clergyman's knee, and miner's elbow, depending on the affected individual's occupation and area of injury.
Causes
The following are some of the more common causes for heel bursitis. Overuse (common in runners and athletes). Running with the wrong footwear. A sudden impact to the foot. Repetitive stress. Underlying inflammatory condition (such as osteoarthritis).
Symptoms
Achiness or stiffness in the affected joint. Worse pain when you press on or move the joint. A joint that looks red and swollen (especially when the bursae in the knee or elbow are affected). A joint that feels warm to the touch, compared to the unaffected joint, which could be a sign that you have an infection in the bursa. A ?squishy? feeling when you touch the affected part. Symptoms that rapidly reappear after an injury or sharp blow to the affected area.
Diagnosis
Obtaining a detailed history from the patient is important in diagnosing calcaneal bursitis. The following complaints (which the physician should ask about during the subjective examination) are commonly reported by patients.
Other inquiries that the physician should make include the following. The clinician should ask about the patient's customary footwear (whether, for example, it includes high-heeled shoes or tight-fitting athletic shoes). The patient should be asked specifically about any recent change in footwear, such as whether he/she is wearing new athletic shoes or whether the patient has made a transition from flat shoes to high heels or vice versa. Individuals who have been accustomed to wearing high-heeled shoes on a long-term basis may find that switching to flat shoes causes increased stretch and irritation of the Achilles tendon and the associated bursae. The specifics of a patient's activity level should be ascertained, including how far the patient runs and, in particular, whether the individual is running with greater intensity than before or has increased the distance being run. The history of any known or suspected underlying rheumatologic conditions, such as gout, rheumatoid arthritis, or seronegative spondyloarthropathies, should be obtained.
Non Surgical Treatment
Treatment is primarily comprised of relief from the painful activity (running). It is important that shoes do not pinch the heel. If satisfactory progress is not made during the rehabilitation, medical treatment can be considered in the form of rheumatic medicine (NSAID) or injection of corticosteroid in the bursa. Injections should be performed under ultrasound guidance to ensure optimal effect and reduce the risk of injecting into the Achilles itself. If progress is not made neither through rehabilitation nor medicinal treatment, surgical treatment can be attempted.
Surgical Treatment
Only if non-surgical attempts at treatment fail, will it make sense to consider surgery. Surgery for retrocalcanel bursitis can include many different procedures. Some of these include removal of the bursa, removing any excess bone at the back of the heel (calcaneal exostectomy), and occasionally detachment and re-attachment of the Achilles tendon. If the foot structure and shape of the heel bone is a primary cause of the bursitis, surgery to re-align the heel bone (calcaneal osteotomy) may be considered. Regardless of which exact surgery is planned, the goal is always to decrease pain and correct the deformity. The idea is to get you back to the activities that you really enjoy. Your foot and ankle surgeon will determine the exact surgical procedure that is most likely to correct the problem in your case. But if you have to have surgery, you can work together to develop a plan that will help assure success.
Bursitis is the painful inflammation of the bursa, a padlike sac found in areas subject to friction. Bursae cushion the movement between the bones, tendons and muscles near the joints. Bursitis is most often caused by repetitive movement and is known by several common names including weaver's bottom, clergyman's knee, and miner's elbow, depending on the affected individual's occupation and area of injury.
Causes
The following are some of the more common causes for heel bursitis. Overuse (common in runners and athletes). Running with the wrong footwear. A sudden impact to the foot. Repetitive stress. Underlying inflammatory condition (such as osteoarthritis).
Symptoms
Achiness or stiffness in the affected joint. Worse pain when you press on or move the joint. A joint that looks red and swollen (especially when the bursae in the knee or elbow are affected). A joint that feels warm to the touch, compared to the unaffected joint, which could be a sign that you have an infection in the bursa. A ?squishy? feeling when you touch the affected part. Symptoms that rapidly reappear after an injury or sharp blow to the affected area.
Diagnosis
Obtaining a detailed history from the patient is important in diagnosing calcaneal bursitis. The following complaints (which the physician should ask about during the subjective examination) are commonly reported by patients.
Other inquiries that the physician should make include the following. The clinician should ask about the patient's customary footwear (whether, for example, it includes high-heeled shoes or tight-fitting athletic shoes). The patient should be asked specifically about any recent change in footwear, such as whether he/she is wearing new athletic shoes or whether the patient has made a transition from flat shoes to high heels or vice versa. Individuals who have been accustomed to wearing high-heeled shoes on a long-term basis may find that switching to flat shoes causes increased stretch and irritation of the Achilles tendon and the associated bursae. The specifics of a patient's activity level should be ascertained, including how far the patient runs and, in particular, whether the individual is running with greater intensity than before or has increased the distance being run. The history of any known or suspected underlying rheumatologic conditions, such as gout, rheumatoid arthritis, or seronegative spondyloarthropathies, should be obtained.
Non Surgical Treatment
Treatment is primarily comprised of relief from the painful activity (running). It is important that shoes do not pinch the heel. If satisfactory progress is not made during the rehabilitation, medical treatment can be considered in the form of rheumatic medicine (NSAID) or injection of corticosteroid in the bursa. Injections should be performed under ultrasound guidance to ensure optimal effect and reduce the risk of injecting into the Achilles itself. If progress is not made neither through rehabilitation nor medicinal treatment, surgical treatment can be attempted.
Surgical Treatment
Only if non-surgical attempts at treatment fail, will it make sense to consider surgery. Surgery for retrocalcanel bursitis can include many different procedures. Some of these include removal of the bursa, removing any excess bone at the back of the heel (calcaneal exostectomy), and occasionally detachment and re-attachment of the Achilles tendon. If the foot structure and shape of the heel bone is a primary cause of the bursitis, surgery to re-align the heel bone (calcaneal osteotomy) may be considered. Regardless of which exact surgery is planned, the goal is always to decrease pain and correct the deformity. The idea is to get you back to the activities that you really enjoy. Your foot and ankle surgeon will determine the exact surgical procedure that is most likely to correct the problem in your case. But if you have to have surgery, you can work together to develop a plan that will help assure success.
Hammertoes Surgery
 Overview
Overview
Uneven muscle tension results in the distortion of one or several of the small toes. (hammertoe) Pressure points develop at the raised middle joint as well as at the tip of the toe and underneath the metatarsal head. In the beginning, when the misalignment can still be corrected, it often suffices to lengthen the tendon and to cut a notch into the capsule. In a contracted misalignment, part of the middle joint is removed to form a replacement joint. Modern surgical techniques preserve the metatarsophalangeal joint (Weil or Helal osteotomies).
Causes
As described above, the main reason people develop hammertoes is improper footwear, or footwear that is too short for the toes. Shoes that do not allow our toes to lie flat are the biggest cause of hammertoes, though there are others, including genetics, injury or trauma in which the toe is jammed or broken. Diseases that affect the nerves and muscles, such as arthritis. Abnormal foot mechanics due to nerve or muscle damage, causing an imbalance of the flexor and extensor tendons of the toe. Systematic diseases such as arthritis can also lead to problems such as hammertoe. Some people are born with hammertoes, while others are more prone to developing the condition due to genetics. If you have ever broken a toe, you know there is not much that can be done for it. It is one of the only bones in the body that heals without the use of a cast. A broken toe may be splinted, however, which may help prevent a hammertoe from forming.
 Symptoms
Symptoms
A toe stuck in an upside-down "V" is probably a hammertoe. Some symptoms are, pain at the top of the bent toe when putting on a shoe. Corns forming on the top of the toe joint. The toe joint swelling and taking on an angry red colour. Difficulty in moving the toe joint and pain when you try to so. Pain on the ball of the foot under the bent toe. Seek medical advice if your feet regularly hurt, you should see a doctor or podiatrist. If you have a hammertoe, you probably need medical attention. Ask your doctor for a referral to a podiatrist or foot surgeon. Act now, before the problem gets worse.
Diagnosis
The treatment options vary with the type and severity of each hammer toe, although identifying the deformity early in its development is important to avoid surgery. Your podiatric physician will examine and X-ray the affected area and recommend a treatment plan specific to your condition.
Non Surgical Treatment
If the affected toe is still flexible, you may be able to treat it by taping or splinting the toe to hold it straight. Your family doctor can show hammertoes you how to do this. You may also try corrective footwear, corn pads and other devices to reduce pain. You may need to do certain exercises to keep your toe joints flexible. For example, you may need to move and stretch your toe gently with your hands. You can also exercise by picking things up with your toes. Small or soft objects, such as marbles or towels, work best. If your hammer toe becomes painful, you may need to apply an ice pack several times a day. This can help relieve the soreness and swelling. Nonsteroidal anti-inflammatory medicines (also called NSAIDs), such as ibuprofen (two brand names: Advil, Motrin) or naproxen (one brand name: Aleve), may be helpful. If your pain and swelling are severe, your doctor may need to give you a steroid injection in the toe joint.
Surgical Treatment
The deformity is corrected in a variety of ways. There are actually a large number of procedures. The simplest procedure would involve a Tenotomy, the cutting of the tendon causing the deformity or a Tendon Lengthening procedure. These procedures are infrequently done, though, as the structural deformity (the arthritis and joint adaptation) is not addressed with these surgeries. Other soft-tissue procedures involve rebalancing the tendons around the joint. There are several techniques to do this, but the most common is probably the Girdlestone-Taylor procedure, which involves rerouting the tendons on the bottom of the toe up and over the toe where it sticks up, so that the tendon helps pull the toe downwards into proper alignment.
Which Are The Primary Causes Of Over-Pronation Of The Foot
Overview
It is estimated that around 80% of the population suffer from excessive pronation. This condition is common in all types of people from children to the elderly and from top athletes to people with a sedentary lifestyle. The feet become misaligned and combined with poor posture roll inwards to gain ground contact, the arches become flattened producing the condition known as excessive pronation. When the feet are excessively pronated a combination of poor posture and diminished shock absorption results in some areas of the feet being subjected to excessive stress and pressure. This can lead to various conditions including knee and back problems, as well as foot problems and deformities.
Causes
Excess stress on the inner surface of the foot can cause injury and pain in the foot and ankle. Repeated rotational forces through the shin, knee, thigh and pelvis also place additional strain on the muscles, tendons and ligaments of the lower leg.
Symptoms
Because pronation is a twisting of the foot, all of the muscles and tendons which run from the leg and ankle into the foot will be twisted. In over-pronation, resulting laxity of the soft tissue structures of the foot and loosened joints cause the bones of the feet shift. When this occurs, the muscles which attach to these bones must also shift, or twist, in order to attach to these bones. The strongest and most important muscles that attach to our foot bones come from our lower leg. So, as these muscles course down the leg and across the ankle, they must twist to maintain their proper attachments in the foot. Injuries due to poor biomechanics and twisting of these muscles due to over-pronation include: shin splints, Achilles Tendonitis, generalized tendonitis, fatigue, muscle aches and pains, cramps, ankle sprains, and loss of muscular efficiency (reducing walking and running speed and endurance). Foot problems due to over-pronation include: bunions, heel spurs, plantar fasciitis, fallen and painful arches, hammer toes, and calluses.
Diagnosis
If you cannot afford to get a proper gait analysis completed, having someone observe you on a treadmill from behind will give you an idea if you are an overpronator. It is possible to tell without observing directly whether you are likely to be an overpronator by looking at your foot arches. Check your foot arch height by standing in water and then on a wet floor or piece of paper which will show your footprint. If your footprints show little to no narrowing in the middle, then you have flat feet or fallen arches. This makes it highly likely that you will overpronate to some degree when running. If you have low or fallen arches, you should get your gait checked to see how much you overpronate, and whether you need to take steps to reduce the level to which you overpronate. Another good test is to have a look at the wear pattern on an old pair of trainers. Overpronators will wear out the outside of the heel and the inside of the toe more quickly than other parts of the shoe. If the wear is quite even, you are likely to have a neutral running gait. Wear primarily down the outside edge means that you are a supinator. When you replace your running shoes you may benefit from shoes for overpronation. Motion control or stability running shoes are usually the best bet to deal with overpronation.
Non Surgical Treatment
Your podiatrist will look at your current footwear to ensure that it is both well-fitted and possessed of adequate cushioning to protect your feet. Firm heel support is advised for over-pronators, and a good fit is important to ensure that the foot as a whole is well supported as instability can exacerbate the existing problems caused by over-pronation.
Surgical Treatment
Hyperpronation can only be properly corrected by internally stabilizing the ankle bone on the hindfoot bones. Several options are available. Extra-Osseous TaloTarsal Stabilization (EOTTS) There are two types of EOTTS procedures. Both are minimally invasive with no cutting or screwing into bone, and therefore have relatively short recovery times. Both are fully reversible should complications arise, such as intolerance to the correction or prolonged pain. However, the risks/benefits and potential candidates vary. Subtalar Arthroereisis. An implant is pushed into the foot to block the excessive motion of the ankle bone. Generally only used in pediatric patients and in combination with other procedures, such as tendon lengthening. Reported removal rates vary from 38% - 100%, depending on manufacturer. HyProCure Implant. A stent is placed into a naturally occurring space between the ankle bone and the heel bone/midfoot bone. The stent realigns the surfaces of the bones, allowing normal joint function. Generally tolerated in both pediatric and adult patients, with or without adjunct soft tissue procedures. Reported removal rates, published in scientific journals vary from 1%-6%.
It is estimated that around 80% of the population suffer from excessive pronation. This condition is common in all types of people from children to the elderly and from top athletes to people with a sedentary lifestyle. The feet become misaligned and combined with poor posture roll inwards to gain ground contact, the arches become flattened producing the condition known as excessive pronation. When the feet are excessively pronated a combination of poor posture and diminished shock absorption results in some areas of the feet being subjected to excessive stress and pressure. This can lead to various conditions including knee and back problems, as well as foot problems and deformities.
Causes
Excess stress on the inner surface of the foot can cause injury and pain in the foot and ankle. Repeated rotational forces through the shin, knee, thigh and pelvis also place additional strain on the muscles, tendons and ligaments of the lower leg.
Symptoms
Because pronation is a twisting of the foot, all of the muscles and tendons which run from the leg and ankle into the foot will be twisted. In over-pronation, resulting laxity of the soft tissue structures of the foot and loosened joints cause the bones of the feet shift. When this occurs, the muscles which attach to these bones must also shift, or twist, in order to attach to these bones. The strongest and most important muscles that attach to our foot bones come from our lower leg. So, as these muscles course down the leg and across the ankle, they must twist to maintain their proper attachments in the foot. Injuries due to poor biomechanics and twisting of these muscles due to over-pronation include: shin splints, Achilles Tendonitis, generalized tendonitis, fatigue, muscle aches and pains, cramps, ankle sprains, and loss of muscular efficiency (reducing walking and running speed and endurance). Foot problems due to over-pronation include: bunions, heel spurs, plantar fasciitis, fallen and painful arches, hammer toes, and calluses.
Diagnosis
If you cannot afford to get a proper gait analysis completed, having someone observe you on a treadmill from behind will give you an idea if you are an overpronator. It is possible to tell without observing directly whether you are likely to be an overpronator by looking at your foot arches. Check your foot arch height by standing in water and then on a wet floor or piece of paper which will show your footprint. If your footprints show little to no narrowing in the middle, then you have flat feet or fallen arches. This makes it highly likely that you will overpronate to some degree when running. If you have low or fallen arches, you should get your gait checked to see how much you overpronate, and whether you need to take steps to reduce the level to which you overpronate. Another good test is to have a look at the wear pattern on an old pair of trainers. Overpronators will wear out the outside of the heel and the inside of the toe more quickly than other parts of the shoe. If the wear is quite even, you are likely to have a neutral running gait. Wear primarily down the outside edge means that you are a supinator. When you replace your running shoes you may benefit from shoes for overpronation. Motion control or stability running shoes are usually the best bet to deal with overpronation.
Non Surgical Treatment
Your podiatrist will look at your current footwear to ensure that it is both well-fitted and possessed of adequate cushioning to protect your feet. Firm heel support is advised for over-pronators, and a good fit is important to ensure that the foot as a whole is well supported as instability can exacerbate the existing problems caused by over-pronation.
Surgical Treatment
Hyperpronation can only be properly corrected by internally stabilizing the ankle bone on the hindfoot bones. Several options are available. Extra-Osseous TaloTarsal Stabilization (EOTTS) There are two types of EOTTS procedures. Both are minimally invasive with no cutting or screwing into bone, and therefore have relatively short recovery times. Both are fully reversible should complications arise, such as intolerance to the correction or prolonged pain. However, the risks/benefits and potential candidates vary. Subtalar Arthroereisis. An implant is pushed into the foot to block the excessive motion of the ankle bone. Generally only used in pediatric patients and in combination with other procedures, such as tendon lengthening. Reported removal rates vary from 38% - 100%, depending on manufacturer. HyProCure Implant. A stent is placed into a naturally occurring space between the ankle bone and the heel bone/midfoot bone. The stent realigns the surfaces of the bones, allowing normal joint function. Generally tolerated in both pediatric and adult patients, with or without adjunct soft tissue procedures. Reported removal rates, published in scientific journals vary from 1%-6%.
How Do I Take Care Of Calcaneal Apophysitis At Home ?
Overview
During AGS, and in specific reference to Sever?s disease, the heel bone grows faster than the Achilles tendon, resulting in an extremely tight Achilles tendon. Because the foot is one of the first parts of the body to grow to full size, and because the heel is not a very flexible area, it is especially susceptible to injury. The Achilles tendon (also called the heel cord) is the strongest tendon that attaches to the growth plate in the heel. Over time, repeated stress (such as impact activities) on the tight Achilles tendon causes the tendon to pull on and damage the growth plate in the heel, resulting in swelling, tenderness, and pain.
Causes
The condition is thought to result from repetitive microtrauma to growth plates of the calcaneus. Although some of the recent articles says, there is no evidence to support that weight and activity levels are risk factors for Sever's disease. High plantar foot pressures are associated with Sever's disease, although it is unclear whether they are a predisposing factor or a result of the condition. Gastrocnemius equinus may be a predisposing factor for Sever's disease.
Symptoms
Signs and symptoms of Sever?s disease include heel pain can be in one or both heels, and it can come and go over time. Many children walk or run with a limp, they may walk on their toes to avoid pressure on their heels. Heel pain may increase with running or jumping, wearing stiff, hard shoes (ex. soccer cleats, flip-flops) or walking barefoot. The pain may begin after increasing physical activity, such as trying a new sport or starting a new sports season.
Diagnosis
This condition is self limiting, it will go away when the two parts of bony growth join together, this is natural. Unfortunately, Sever's disease can be very painful and limit sport activity of the child while waiting for it to go away, so treatment is often advised to help relieve it. In a few cases of Sever's disease, the treatment is not successful and these children will be restricted in their activity levels until the two growth areas join, usually around the age of 16 years. There are no known long term complications associated with Sever's disease.
Non Surgical Treatment
In general, management is along the normal lines for sports injuries. Simply telling an individual to give up his or her chosen sport is not satisfactory (this may be a very talented young footballer who hopes to become a professional). Explain to the child and parent that this is an overuse injury, common in the growing child. It has a good prognosis but it is necessary to ease back on training for a while to let it recover. Offer to talk to the coach. If the parent and coach are one and the same, beware that the child is being 'pushed' too hard. During abstinence from normal training, cardiovascular fitness can be maintained by non-weight-bearing exercise such as swimming or cycling.
Exercise
Stretching exercises can help. It is important that your child performs exercises to stretch the hamstring and calf muscles, and the tendons on the back of the leg. The child should do these stretches 2 or 3 times a day. Each stretch should be held for about 20 seconds. Both legs should be stretched, even if the pain is only in 1 heel. Your child also needs to do exercises to strengthen the muscles on the front of the shin. To do this, your child should sit on the floor, keeping his or her hurt leg straight. One end of a bungee cord or piece of rubber tubing is hooked around a table leg. The other end is hitched around the child's toes. The child then scoots back just far enough to stretch the cord. Next, the child slowly bends the foot toward his or her body. When the child cannot bend the foot any closer, he or she slowly points the foot in the opposite direction (toward the table). This exercise (15 repetitions of "foot curling") should be done about 3 times. The child should do this exercise routine a few times daily.
During AGS, and in specific reference to Sever?s disease, the heel bone grows faster than the Achilles tendon, resulting in an extremely tight Achilles tendon. Because the foot is one of the first parts of the body to grow to full size, and because the heel is not a very flexible area, it is especially susceptible to injury. The Achilles tendon (also called the heel cord) is the strongest tendon that attaches to the growth plate in the heel. Over time, repeated stress (such as impact activities) on the tight Achilles tendon causes the tendon to pull on and damage the growth plate in the heel, resulting in swelling, tenderness, and pain.
Causes
The condition is thought to result from repetitive microtrauma to growth plates of the calcaneus. Although some of the recent articles says, there is no evidence to support that weight and activity levels are risk factors for Sever's disease. High plantar foot pressures are associated with Sever's disease, although it is unclear whether they are a predisposing factor or a result of the condition. Gastrocnemius equinus may be a predisposing factor for Sever's disease.
Symptoms
Signs and symptoms of Sever?s disease include heel pain can be in one or both heels, and it can come and go over time. Many children walk or run with a limp, they may walk on their toes to avoid pressure on their heels. Heel pain may increase with running or jumping, wearing stiff, hard shoes (ex. soccer cleats, flip-flops) or walking barefoot. The pain may begin after increasing physical activity, such as trying a new sport or starting a new sports season.
Diagnosis
This condition is self limiting, it will go away when the two parts of bony growth join together, this is natural. Unfortunately, Sever's disease can be very painful and limit sport activity of the child while waiting for it to go away, so treatment is often advised to help relieve it. In a few cases of Sever's disease, the treatment is not successful and these children will be restricted in their activity levels until the two growth areas join, usually around the age of 16 years. There are no known long term complications associated with Sever's disease.
Non Surgical Treatment
In general, management is along the normal lines for sports injuries. Simply telling an individual to give up his or her chosen sport is not satisfactory (this may be a very talented young footballer who hopes to become a professional). Explain to the child and parent that this is an overuse injury, common in the growing child. It has a good prognosis but it is necessary to ease back on training for a while to let it recover. Offer to talk to the coach. If the parent and coach are one and the same, beware that the child is being 'pushed' too hard. During abstinence from normal training, cardiovascular fitness can be maintained by non-weight-bearing exercise such as swimming or cycling.
Exercise
Stretching exercises can help. It is important that your child performs exercises to stretch the hamstring and calf muscles, and the tendons on the back of the leg. The child should do these stretches 2 or 3 times a day. Each stretch should be held for about 20 seconds. Both legs should be stretched, even if the pain is only in 1 heel. Your child also needs to do exercises to strengthen the muscles on the front of the shin. To do this, your child should sit on the floor, keeping his or her hurt leg straight. One end of a bungee cord or piece of rubber tubing is hooked around a table leg. The other end is hitched around the child's toes. The child then scoots back just far enough to stretch the cord. Next, the child slowly bends the foot toward his or her body. When the child cannot bend the foot any closer, he or she slowly points the foot in the opposite direction (toward the table). This exercise (15 repetitions of "foot curling") should be done about 3 times. The child should do this exercise routine a few times daily.